For home health and hospice leaders, scheduling has become an economic control system.
Workforce shortages, regulatory timing requirements, rising labor costs, and fuel volatility converge to make scheduling a primary lever for capacity, margin protection, and risk mitigation. For COOs and VPs of Operations, the question is no longer whether scheduling can be optimized. The question is whether your current approach can withstand today’s structural pressures.
The influence of home health agency scheduling software is increasing as systems modernize. The ability to centralize and standardize scheduling practices helps determine whether agencies can scale predictably. Scalability barriers often lead to growth plateaus because of administrative strain.
The economic forces reshaping scheduling in home-based care
Workforce shortages are structural, not temporary
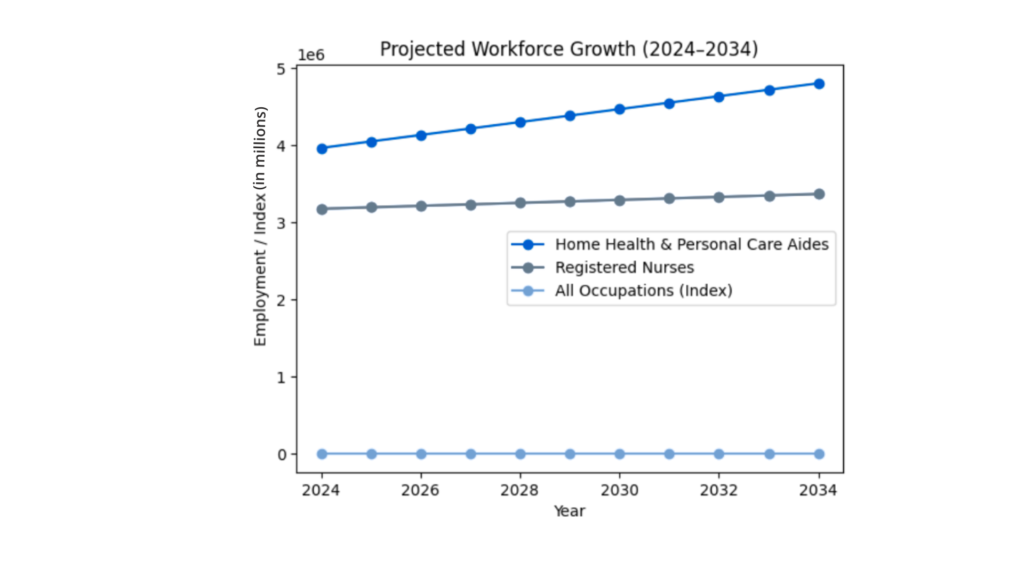
Demand for home-based care is rising rapidly as the U.S. population ages. The U.S. Census Bureau projects that by 2030, one in five Americans will be age 65 or older, a demographic shift that significantly expands demand for home health, hospice, and personal care services.
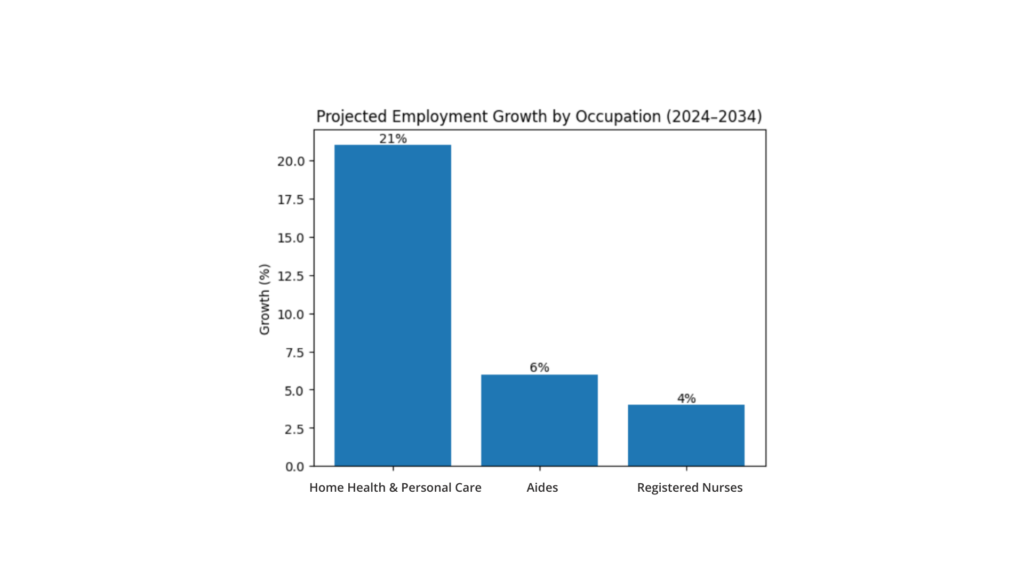
At the same time, workforce supply remains constrained. According to the U.S. Bureau of Labor Statistics, employment for home health and personal care aides is projected to grow 21% between 2024 and 2034, far faster than the average for all occupations.
While this reflects rising demand, it also highlights the structural challenge: agencies must scale care delivery while competing for a limited labor pool.
Some visible impacts across organizations include:
- Difficulty recruiting nurses and therapists
- Increased overtime costs
- Higher reliance on contract staff
- Growing administrative workloads for schedulers
Manual scheduling environments amplify these pressures. Without structured automation and guardrails, schedulers spend significant time struggling to keep up with routine tasks and last minute requests instead creating optimized schedules.
When growth increases complexity faster than operational systems can absorb it, scheduling becomes the bottleneck.
Regulatory timing dictates visit execution — not preference
Scheduling in home-based care is not discretionary. It is regulated.
Home health: PDGM and LUPA implications
Under the Home Health Prospective Payment System (PDGM), Low Utilization Payment Adjustment (LUPA) thresholds vary based on case-mix groups. When visits fall below the threshold, reimbursement shifts from episodic payment to per-visit reimbursement.
This means visit timing and completion directly influence financial performance.
Missed or poorly sequenced visits can:
- Trigger avoidable LUPAs or outliers
- Reduce reimbursement
- Create documentation risk
- Increase audit exposure
PDGM reimbursement rules make visit execution discipline essential because scheduling errors have financial consequences.
Hospice: HOPE raises the bar for visit timing and documentation
Hospice agencies have faced a similar shift. Beginning October 1, 2025, the Hospice Outcomes & Patient Evaluation (HOPE) assessment replaced the Hospice Item Set (HIS).
HOPE introduced expanded clinical data capture and timing expectations tied to symptom follow-up, visit documentation, and quality reporting.
In practical terms, hospice scheduling must support:
- Proper timing for Hospice Utilization Visits (HUV)
- Proper timing for Symptom follow up visits (SFV)
- Frequency coordination schedulers and clinicians
In both service lines, medical scheduling has become a compliance-sensitive workflow that must be supported by analytics data to track compliance.
Rising costs amplify the operational stakes
Labor is not the only economic variable affecting scheduling. Transportation costs and traffic also influence productivity.
Home-based care clinicians spend a large portion of their workday traveling between patients. When routing is inefficient:
- Drive time expands
- Productivity decreases
- Overtime increases
- Burnout accelerates
Small inefficiencies multiply across thousands of visits per month. At the same time, wage pressure continues to rise. According to the U.S. Bureau of Labor Statistics, the median annual wage for home health and personal care aides has increased from about $27,080 in 2020 to roughly $33,530 today (around $16 per hour), reflecting the growing demand for these roles as agencies compete for a limited workforce. Wage pressure is increasing for skilled clinicians as well. The median annual wage for registered nurses has risen from about $75,330 in 2020 to approximately $93,600 in 2024, reflecting the growing demand for nursing talent across healthcare settings, including home-based care.
Medicare Advantage growth adds operational complexity
The payer landscape is also shifting. According to the Centers for Medicare & Medicaid Services (CMS), more than half of all Medicare beneficiaries are now enrolled in Medicare Advantage plans.
Medicare Advantage often introduces:
- Prior authorization requirements
- Visit frequency review
- Documentation variability
- Authorization delays
These administrative steps can affect scheduling windows and visit timing, increasing coordination complexity for operations teams. Scheduling systems must now account for payer workflows as well as clinical workflows.
Why scheduling optimization is an executive strategy
Modern home healthcare scheduling software must function as an operational control system, not a digital calendar. Effective scheduling technology supports:
- Discipline-specific visit rules
- Timing guidelines for LUPAs
- HOPE visit timing expectations
- Clinician licensure and productivity standards
- Territory and routing guardrails
- Patient preferences and availability
Scheduling rules are highly customized by visit type, discipline, and diagnosis. Operational clarity must exist before automation can scale it. Technology cannot compensate for undefined processes. But once processes are defined, automation can create operational consistency across branches.
Scheduling stability supports clinician retention
Operational stability also improves workforce sustainability. Unpredictable schedules, late changes, and uneven workloads are leading drivers of clinician burnout.
When clinicians have advance visibility into their schedules and fewer last-minute changes, job satisfaction improves.
Technology cannot solve workforce shortages alone, but it can remove operational friction that contributes to turnover.
Automation as a capacity unlock
When configured with clear operational guardrails, Smart Scheduling can help agencies automate significant portions of the scheduling process.
The system is capable of:
- Scheduling up to 95% of visit types
- Automating up to 65% of visits depending on configuration
- Completing up to 20% of workflow tasks with zero touches
Configuration choices, operational discipline, and exception management create a tailored scheduling experience using a two-speed automation model that balances stability with responsiveness.
Forward-looking scheduling
Nightly automation can schedule visits seven to fifteen days in advance based on defined guardrails. This forward planning helps stabilize clinician schedules, balance workloads, and reduce reactive rescheduling which improves visibility and predictability for field staff.
Real-time dispatching
Home-based care is dynamic, and same-day adjustments are often needed due to missed visits, patient requests, or new clinical needs. Real-time dispatch allows the system to recommend schedule changes while maintaining human approval. Semi-automated workflows and clinician push notifications ensure updates are communicated quickly without sacrificing operational control.
Together, forward-looking automation and real-time dispatching allow schedulers to focus on managing exceptions rather than manually placing visits.
The financial lens: from scheduling chaos to operational clarity
For COOs and VPs of Operations, scheduling optimization must translate into measurable operational improvements.
Potential areas of impact include:
- Increased average daily census coverage per scheduler
- Reduced scheduler recruiting needs
- Lower overtime exposure
- Fewer avoidable LUPAs
- Easier HOPE compliance
- Improved start-of-care timeliness
Scheduling does not eliminate necessary care. Instead, it supports delivering the right care at the right time with operational consistency.
The strategic shift: from coordination to orchestration
Agencies that treat scheduling as clerical coordination will struggle to scale under today’s economic conditions. Agencies that treat scheduling as operational infrastructure will be better positioned to:
- Protect margin
- Expand capacity
- Manage regulatory complexity
- Improve workforce stability
- Maintain referral confidence
Home health agency scheduling software is no longer about filling time slots. It is about enabling operational resilience.
Taking the next step
If your organization is evaluating how to scale operations without increasing administrative strain, learn more about how Smart Scheduling supports configurable guardrails, automation, and operational clarity.
You can also request more information here to explore how scheduling optimization fits into your growth strategy.