Why home healthcare growth is being limited by operations, not referrals
If you are a CEO or COO in home-based care, demand is not your biggest concern.
What keeps leaders up at night is whether their organization can reliably turn referrals into admits, deliver care on time, document it defensibly, and bill it accurately without exhausting clinicians or destabilizing cash flow.
That is the central finding of The State of Home-Based Care in 2026: access to care is increasingly constrained by operational capacity, not patient demand.
One of the clearest indicators shows up early in the care journey. Referral conversion rates have declined 13 percent since 2018, dropping from 77 percent to 64 percent by Q2 2025, even as overall census continues to grow.
This reality reframes the access-to-care conversation for executive leaders. Growth is no longer limited by referrals or reputation. Heading into 2026, under rising oversight and payer complexity, growth is limited by how effectively intake, start of care, documentation, and billing operate together as a connected system.
The demand wave is real and the tide is still rising
Demographics continue to drive sustained demand for home health and hospice services.
By 2030, all Baby Boomers will be older than 65, and one in five Americans will be of retirement age. CMS data already reflects the impact: more than 11,000 Medicare-certified home health agencies serve approximately 3 million Medicare fee-for-service beneficiaries each year, with utilization continuing to rise.
Workforce constraints, however, remain unresolved. The Bureau of Labor Statistics projects 17 percent growth in home health and personal care aide employment through 2034, with hundreds of thousands of openings each year. Demand and labor pressure are increasing at the same time.
Demand is not the limiting factor. The constraint is whether agencies can unlock more capacity despite staffing shortages and growing payer complexity.
Capacity in home healthcare is a throughput system
When leaders say, “We don’t have capacity,” they often mean staffing.
But capacity is being lost long before staffing becomes the issue. It is lost across a chain of handoffs that determine whether demand becomes revenue or becomes a denied referral.
Capacity is best understood as a system:
Capacity equals the referrals you can accept, the starts you can schedule, the visits you can deliver, the documentation you can complete, and the claims you can bill and collect—within required timeframes.
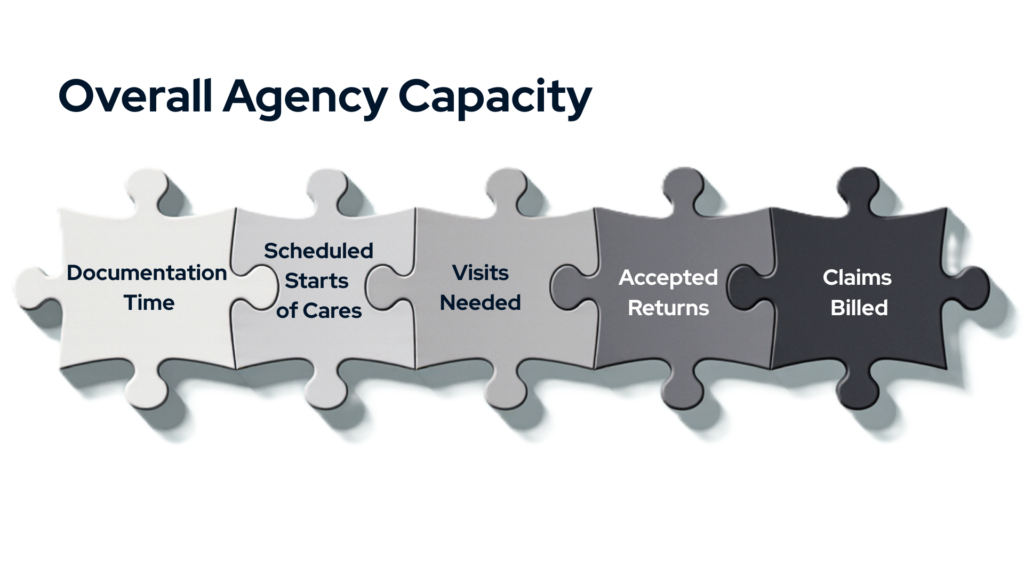
When any part of that system slows down, overall capacity shrinks.
Where capacity is being lost in 2026
The 2026 industry data points to four consistent pressure points where capacity leakage occurs: intake, start of care, documentation, and billing.
Intake is the first capacity gate
Referral volume does not equal growth. Conversion does.
The sustained decline in referral conversion is an operational warning sign. When organizations cannot evaluate, qualify, authorize, and schedule efficiently, demand turns into capacity they cannot access.
Common sources of intake leakage include slow accept or decline decisions, missing information and referral back-and-forth, payer-specific authorization requirements, and late validation of staffing coverage.
When intake is treated as administrative overhead instead of a production system, organizations pay for demand they cannot monetize.
Start-of-care timeliness sets the growth ceiling
Start of care is not just a clinical milestone. It is a throughput lever.
Industry benchmarks show that the median time from referral entry to start of care exceeds 69 hours, with more than 13 hours spent inside intake processes alone. Every delay compounds downstream strain, compressed schedules, care quality challenges, patient fall-off risk, and referral source dissatisfaction.
Documentation is business critical
In 2026, documentation accuracy and timeliness have become executive-level issues.
Incomplete or late documentation creates rework, billing delays, and audit exposure. Under Medicare Advantage and increased hospice oversight, documentation gaps show up as margin erosion and cash flow variability.
Organizations improve documentation efficiency and accuracy protect both capacity and reimbursement.
Billing performance determines what the organization can afford
Cash flow limits capacity. CMS finalized a 1.3 percent reduction in aggregate Medicare payments to home health agencies for CY 2026. When reimbursement tightens while operational friction increases, organizations cannot grow their way out of pressure. The path forward is through operational disciple and execution.
Billing performance directly affects staffing flexibility, technology investment, and growth optionality.
Medicare Advantage is the operating reality
With more than half of eligible Medicare beneficiaries now enrolled in Medicare Advantage, growth and access increasingly depend on how well organizations adapt their operating model to payer-specific requirements. Leading agencies are responding by standardizing intake and authorization workflows, building repeatable payer playbooks, and using data to understand the true cost and timing of care delivery by plan.
Medicare Advantage reshapes how leaders approach documentation, scheduling, and revenue cycle performance—not as isolated functions, but as connected disciplines that determine how many patients the organization can safely and reliably serve.
Hospice oversight is rising—and defensible execution is the baseline
Hospice leaders face parallel pressure.
CMS’s FY 2026 Hospice Wage Index and Payment Rate Update reinforces expectations around documentation accuracy, quality reporting, and audit readiness. Oversight is increasing, and performance will favor organizations that treat compliance as daily execution, not periodic cleanup.
In 2026, hospice success depends on operating quality and compliance as a measurable system.
What to do when demand is strong but capacity is constrained
Once leaders recognize that access-to-care challenges are operational, the question changes. It is no longer, “How do we get more referrals?” It becomes, “Where is capacity leaking today, and how do we reclaim it safely?” The organizations making progress are not chasing volume. They are tightening execution across the system they already have.
Make capacity visible
Capacity strain is often felt before it is measured.
Establish a small set of executive-level indicators that reflect real throughput, such as referral conversion by payer, time to start of care, documentation timeliness, authorization turnaround, clean claim rates, and days in accounts receivable.
The goal is not more reporting. It is shared visibility into where capacity is created or lost each week.
Treat intake, authorization, and start of care as one system
Operationally, intake, authorization, and start of care are inseparable.
Leaders reduce friction by clarifying ownership, tightening decision timelines, and standardizing payer-specific workflows. Fewer handoffs and clearer accountability prevent progress from stalling before care begins.
Reframe documentation as a throughput issue
Documentation determines whether care can move forward.
Setting clear standards for completeness and indicators such as timeliness, rework rates, and audit readiness allows documentation to support flow instead of interrupting it. Setting these standards can also help highlight where additional support from technology or process optimization needs to take place. It also helps tie ROI more closely to documentation efficiency improvements.
Protect clinician time
Clinician time is the most constrained resource in the system. Capacity gains increasingly come from reducing administrative burdens, streamlining documentation workflows, and preventing avoidable rework.
Why this matters now
With reimbursement pressure continuing into 2026, operational excellence is no longer optional. In 2026, stability will favor organizations that understand capacity as a connected system, measure throughput instead of activity, reduce friction, and execute in ways that are defensible under payer and regulatory scrutiny.
A deeper look at capacity, backed by industry data
This blog outlines the capacity challenge leaders are feeling today. Homecare Homebase examines the full picture, how widespread it is, where it shows up most consistently, and how organizations are responding in a comprehensive industry report.
The State of Home-Based Care in 2026 brings together national benchmarks, operational metrics, and payer dynamics to help leaders pressure-test priorities and plan with clarity.
Download The State of Home-Based Care in 2026
https://hchb.com/2026industryreport/