Home health staffing shortages are no longer a temporary disruption. They are a structural reality reshaping how agencies operate, grow, and deliver care.
For COOs and Chief Clinical Officers, the challenge is not demand. Demand for home-based care continues to rise as the U.S. population ages and payers push care into lower-cost settings. The real constraint is time. Clinician time. Manager time. Administrative time.
According to The State of Home-Based Care in 2026, workforce shortages have fundamentally changed the equation. Agencies cannot hire their way out of today’s capacity challenges without worsening burnout, compliance risk, and margin pressure. The organizations that will outperform in 2026 are shifting focus from headcount to throughput, productivity, and administrative burden reduction.
Why hiring alone won’t solve home health staffing shortages
National workforce data illustrates the scale of the problem. The U.S. Bureau of Labor Statistics projects home health and personal care aide employment will grow 17 percent from 2024 to 2034, with more than 765,000 openings per year on average. Registered nurse demand continues to rise as well, adding nearly 195,000 openings annually. Even under optimistic assumptions, workforce supply will lag demand for years.
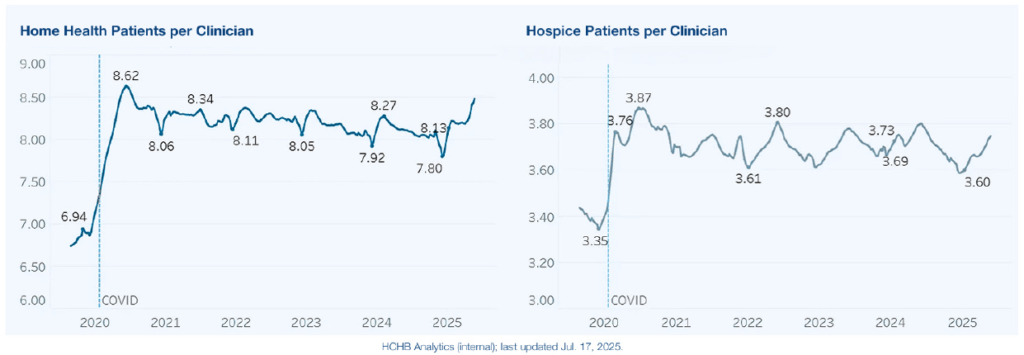
But the more immediate operational reality is this: adding patients per clinician only works up to a point.
The report shows that agencies have increased census by stretching clinician capacity, often by increasing visits per episode or compressing schedules. This approach has limits. Burnout rises. Turnover accelerates. Referral conversion declines. In 2024 alone, more than 4.2 million patients did not receive home health services recommended by their physician, largely due to capacity constraints tied to staffing and operations.
The takeaway for executive leaders is clear. Workforce shortages are not just a recruiting issue. They are an operational throughput problem.
Time is now the scarcest resource in home-based care
The report identifies clinician time as the binding constraint for growth. Capacity is limited not only by clinician availability, but by drive time, scheduling inefficiencies, documentation burden, and administrative rework.
As Medicare Advantage expands and regulatory oversight intensifies, these time drains compound. Prior authorizations delay starts of care. Documentation variability increases rework. Complex compliance requirements add steps without removing old ones. Every minute lost upstream ripples downstream into missed visits, delayed billing, and strained referral relationships.
Kaiser Family Foundation data cited in the report shows Medicare Advantage plans processed nearly 50 million prior authorization requests in a single year, with denials and delays a common issue affecting post-acute services. Even when denials are overturned, the time cost to agencies is real and persistent.
In this environment, time has become the most valuable and least renewable asset agencies have.
Productivity, not staffing ratios, determines capacity
One of the most important shifts highlighted in the report is how leading agencies are redefining productivity.
Productivity is no longer measured only by visits per clinician. It is measured by how efficiently the entire system moves from referral to final billing. Start-of-care timeliness, visit execution, documentation completeness, and revenue cycle accuracy now directly determine how many patients an agency can serve without adding staff.
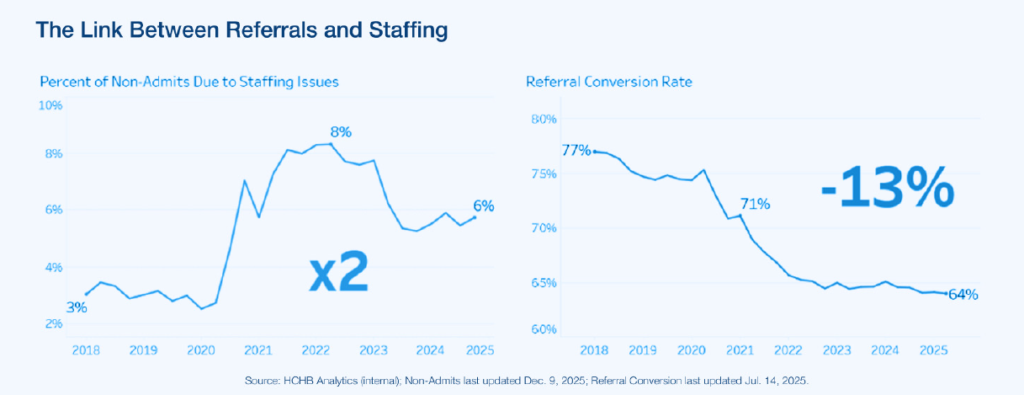
Homecare Homebase analytics cited in the report show referral conversion rates have declined 13 percent since 2018, even as census continues to rise. This divergence signals that demand is outpacing agencies’ operational ability to absorb it.
Agencies reclaiming capacity are focusing on:
- Reducing intake and authorization cycle time
- Minimizing after-hours documentation
- Optimizing scheduling and routing to reduce drive time
- Standardizing workflows to eliminate rework and audit risk
These are time strategies, not hiring strategies.
Administrative burden fuels clinician burnout
Clinician burnout is often discussed as an emotional or cultural issue. The report reframes it as an operational one.
After-hours documentation, inefficient routing, and inconsistent workflows push work into evenings and weekends. This erodes clinician satisfaction and accelerates turnover, especially in the first year of employment when attrition risk is at its highest.
The report emphasizes that documentation efficiency must be paired with compliance rigor. Faster documentation that creates denials or audit exposure simply shifts work from clinicians to back-office teams and undermines margins.
Agencies making progress are embedding documentation support into daily workflows, using analytics to identify burnout risk early, and eliminating low-value administrative tasks that consume clinician time without improving care.
Why technology is now a workforce strategy
Technology adoption is no longer about innovation optics. It is a workforce survival strategy.
The report outlines how agencies are using automation and embedded intelligence to give time back to clinicians without sacrificing care quality or regulatory defensibility. Examples include intake automation to reduce referral-to-admit delays, scheduling optimization to minimize drive time and missed visits, and workflow-native documentation support to reduce after-hours charting.
Importantly, the report cautions against technology that simply shifts work from clinicians to office staff or bypasses clinical judgment. Sustainable gains come from tools that reduce friction across both field and office workflows while maintaining human oversight.
What leaders should prioritize now
For COOs and Chief Clinical Officers, the implications are strategic.
The question for 2026 is not whether workforce shortages will ease. The question is whether your operation can reclaim enough time to serve more patients with the clinicians you already have.
The agencies best positioned for the year ahead are:
- Treating intake, scheduling, care delivery, documentation, and billing as a single connected system
- Measuring time loss as rigorously as financial leakage
- Investing in workflow standardization and automation before adding headcount
- Using analytics to detect burnout risk before turnover occurs
These priorities reflect a shift from reactive staffing decisions to proactive operational design.
Get the full executive analysis
Download the 2026 executive report to get a clear, data-informed view of how workforce shortages, Medicare Advantage, and regulatory pressure are reshaping home-based care, and where leading agencies are reclaiming time without sacrificing care quality or compliance.

Or, if you’re evaluating your own readiness, see how your agency compares heading into 2026 and understand the operational priorities separating organizations that can grow from those that will remain constrained.
The full report translates regulatory, payer, and workforce complexity into practical operational guidance for home health and hospice leaders navigating the year ahead.